Patient Progress Notes Template Word – A Comprehensive Guide for Healthcare Professionals
The consistent and accurate documentation of patient progress is paramount to effective patient care. Patient Progress Notes are a vital tool for clinicians, nurses, and other healthcare providers, enabling them to monitor patient conditions, track treatment effectiveness, and communicate vital information to other members of the healthcare team. Choosing the right format – a standardized patient progress note template – streamlines this process, ensuring clarity, completeness, and ease of access. This article will delve into the importance of patient progress notes, explore different template options, and provide a detailed guide to creating effective and informative notes. Understanding the nuances of these notes is crucial for improving patient outcomes and fostering a collaborative healthcare environment. The core of a successful patient progress note lies in its ability to accurately reflect the patient’s current status, any interventions performed, and the observed changes. It’s more than just a record; it’s a communication tool.
The benefits of utilizing a standardized patient progress note template extend far beyond simple record-keeping. It promotes continuity of care, allowing healthcare providers to quickly access a patient’s history and current status, regardless of where they are in their treatment journey. This is particularly important in complex cases or when multiple healthcare professionals are involved. Furthermore, a well-structured progress note facilitates informed decision-making, enabling clinicians to adjust treatment plans based on real-time observations. It also contributes to improved patient safety by reducing the risk of errors and ensuring that all relevant information is captured. Ultimately, investing in a robust patient progress note system demonstrates a commitment to quality patient care and enhances the overall efficiency of the healthcare organization. The ability to quickly and accurately document patient progress is a significant advantage in today’s demanding healthcare landscape.

Before diving into the specifics of template design, it’s essential to grasp why these notes are so critical. They are the cornerstone of patient-centered care, providing a detailed account of a patient’s condition and response to treatment. They go beyond simply recording events; they capture the why behind the events. This allows for a deeper understanding of the patient’s needs and facilitates proactive interventions. Without thorough progress notes, it’s difficult to identify potential problems early on, leading to delayed or inappropriate treatment. Moreover, they are a vital component of regulatory compliance, ensuring accurate and complete documentation for reporting purposes. The ability to demonstrate adherence to established protocols and guidelines is increasingly important for maintaining accreditation and securing reimbursement. A lack of standardized documentation can lead to legal issues and jeopardize patient safety.
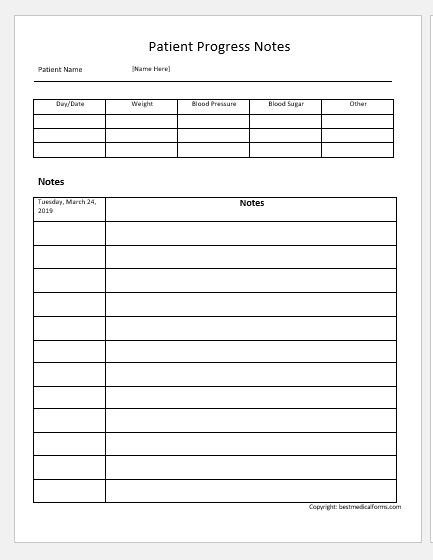
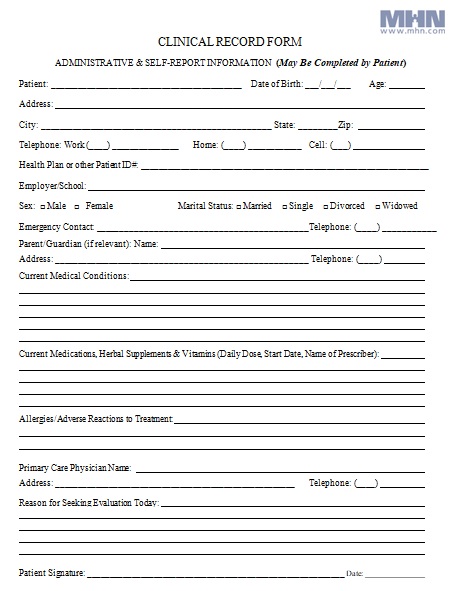
Several different template formats exist, each with its own strengths and weaknesses. The most common options include:
Choosing the right template depends on the specific clinical setting, the type of patient, and the clinician’s preferences. It’s important to select a template that is both comprehensive and easy to use. Many EHR systems offer templates that can be adapted to fit individual patient needs. Furthermore, consistency in documentation is key – adhering to a consistent format across all progress notes ensures that information is readily accessible and comparable.
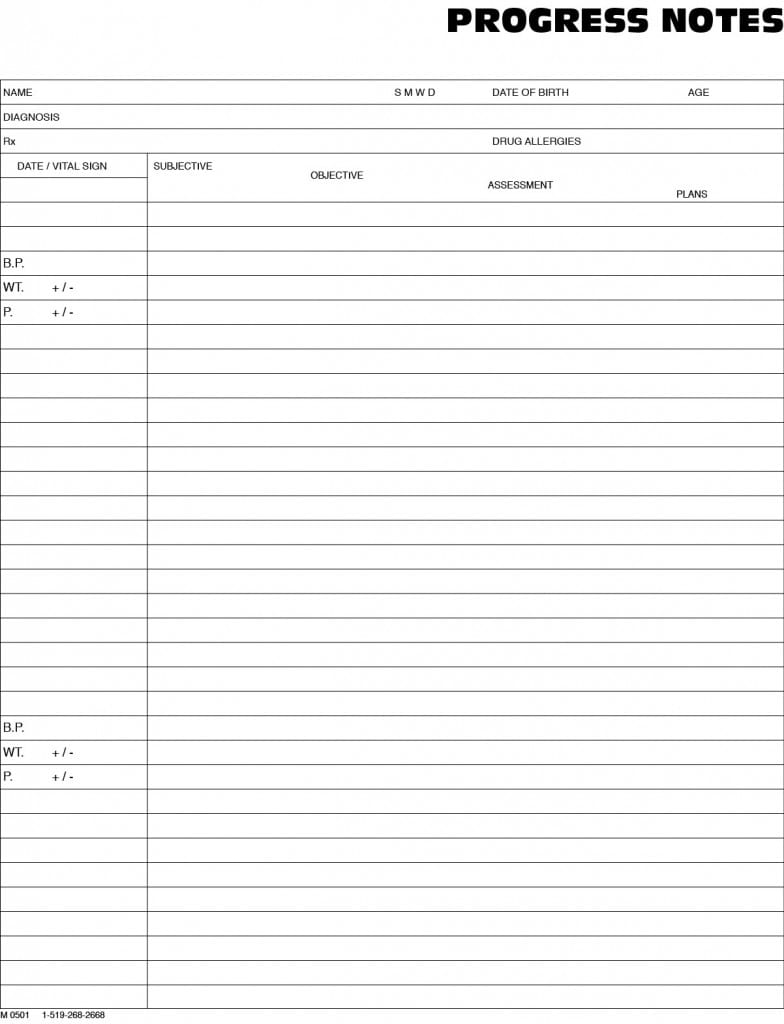
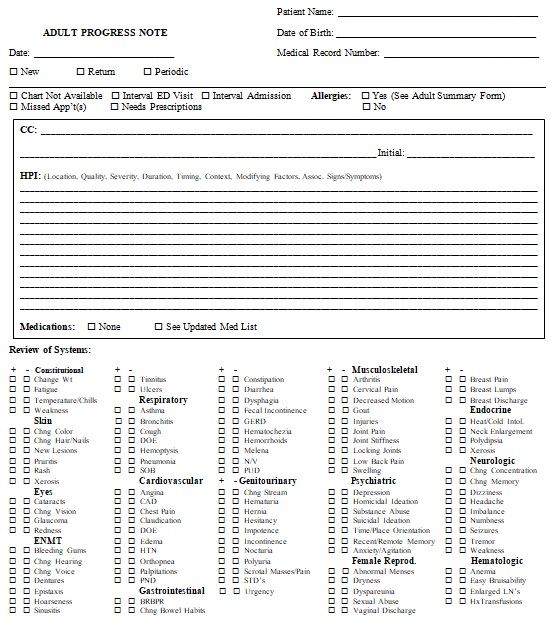
The subjective data section of a patient progress note is where clinicians gather information about the patient’s current state. This involves actively listening to the patient, asking open-ended questions, and carefully observing their responses. It’s not just about recording what the patient says; it’s about understanding their perspective and identifying any potential concerns. Key elements of this section include:
The objective data section focuses on collecting factual information about the patient’s condition. This involves using observation, measurement, and assessment tools to document the patient’s physical and functional status. It’s crucial to be objective and avoid subjective interpretations.
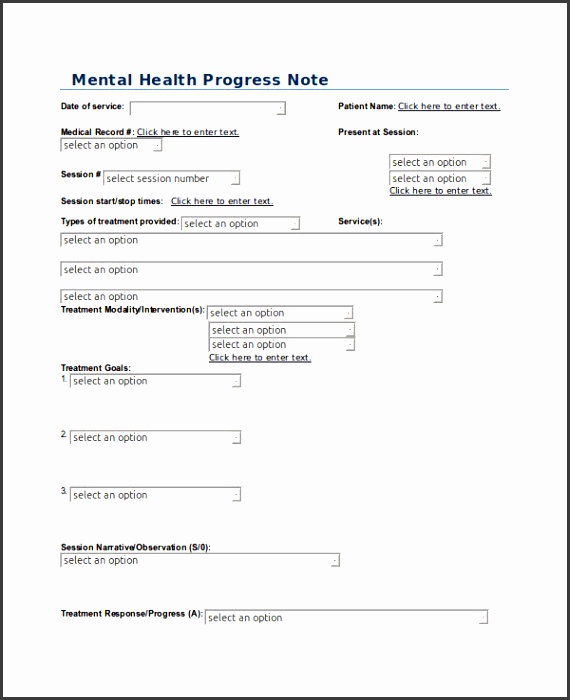
The assessment section is where clinicians synthesize the subjective and objective data to arrive at a diagnosis or treatment plan. This involves identifying patterns, drawing conclusions, and formulating a differential diagnosis. It’s a critical step in ensuring that the patient’s condition is accurately understood.
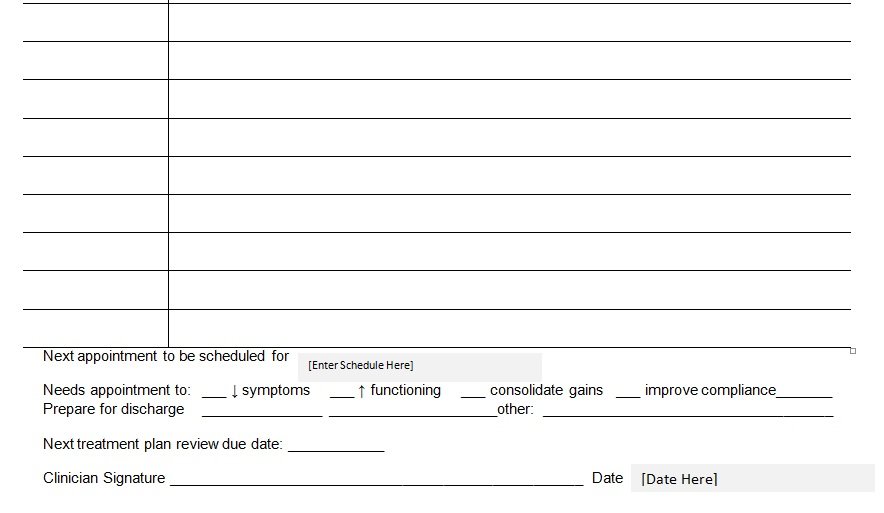
The plan section outlines the specific actions that will be taken to address the patient’s condition. It should be realistic, achievable, and tailored to the patient’s individual needs.
Patient progress notes are an indispensable component of quality patient care. By utilizing a standardized template, gathering accurate data, and documenting the patient’s response to treatment, clinicians can ensure that patients receive the best possible care. The consistent application of these notes facilitates effective communication, improves patient outcomes, and contributes to a more efficient and collaborative healthcare environment. Remember that the key to a successful patient progress note is accuracy, completeness, and a focus on the patient’s needs. Continuous improvement and adaptation of templates are essential to meet the evolving needs of the healthcare system. Investing in training and resources for clinicians to effectively utilize these notes is a worthwhile investment in patient well-being.