Effective medical documentation is the cornerstone of quality patient care, legal compliance, and efficient healthcare operations. In an environment where precise record-keeping is not just a best practice but a legal and ethical imperative, tools that streamline this process are invaluable. One such critical tool is the Soap Report Template, a structured framework designed to ensure comprehensive and consistent clinical notes. By organizing patient information into four distinct categories—Subjective, Objective, Assessment, and Plan—this template empowers healthcare professionals to capture vital data in a standardized, easily digestible format, significantly enhancing communication and continuity of care across various disciplines.
The standardization offered by a well-designed template helps to mitigate common errors associated with free-form note-taking, such as omissions, inconsistencies, or lack of clarity. This structured approach not only saves time during documentation but also makes retrieving and understanding patient information far more efficient for other healthcare providers involved in the patient’s treatment. Ultimately, the systematic nature of this reporting method contributes directly to improved patient safety and better overall health outcomes, as it facilitates a holistic view of the patient’s condition and treatment journey.
Moreover, in an era of increasing legal scrutiny and evolving regulatory requirements, detailed and accurate documentation is paramount. A robust template acts as a guide, ensuring that all necessary information is consistently included, thereby strengthening the legal defensibility of clinical records. It promotes a systematic thought process, encouraging clinicians to move from initial patient complaints through observable findings, a professional diagnosis, and finally to a clear, actionable treatment strategy. This structured approach fosters a higher level of clinical reasoning and accountability.
Beyond its utility in direct patient care and legal protection, the template also serves as an educational tool. For students and new practitioners, it provides a clear framework for learning how to organize clinical information logically and comprehensively. This early adoption of structured documentation practices helps to build a strong foundation for a career in healthcare, where clear and concise record-keeping remains a perpetual necessity. Its adaptability across different specialties further underscores its universal value in the diverse landscape of modern healthcare.
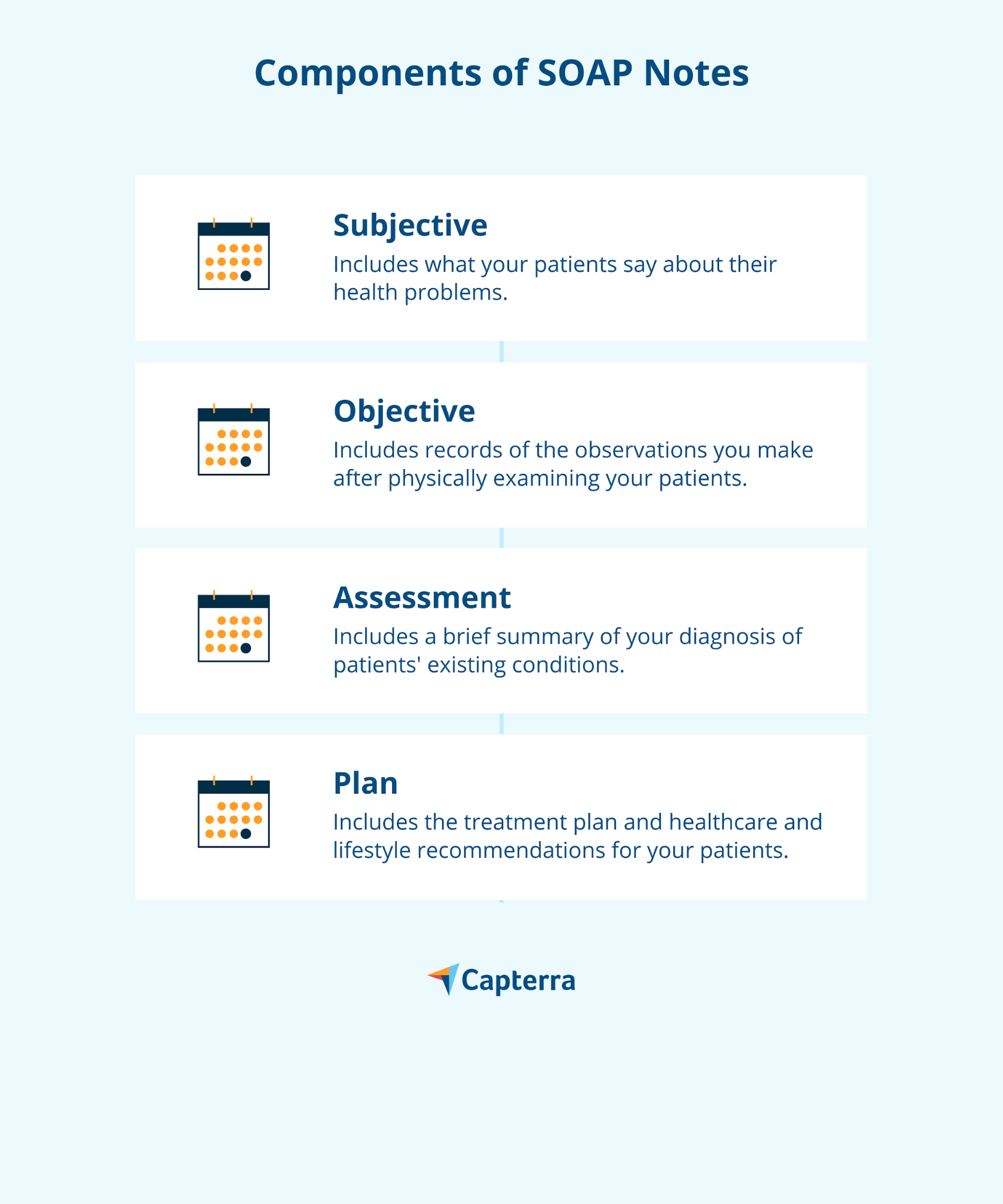
The SOAP note framework is a universally recognized method for documenting patient encounters, providing a structured and systematic approach to clinical record-keeping. Each letter in SOAP represents a distinct section, guiding the practitioner through a logical sequence of information gathering and clinical reasoning. Understanding each component is fundamental to utilizing any Soap Report Template effectively, ensuring that all relevant aspects of a patient’s visit are thoroughly documented.
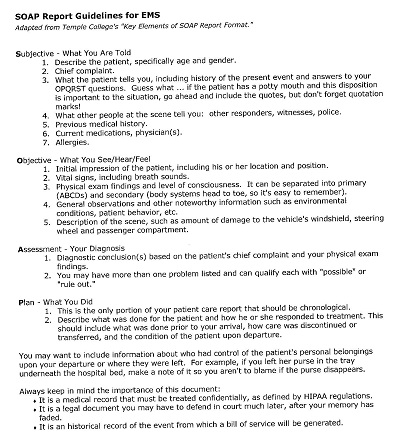
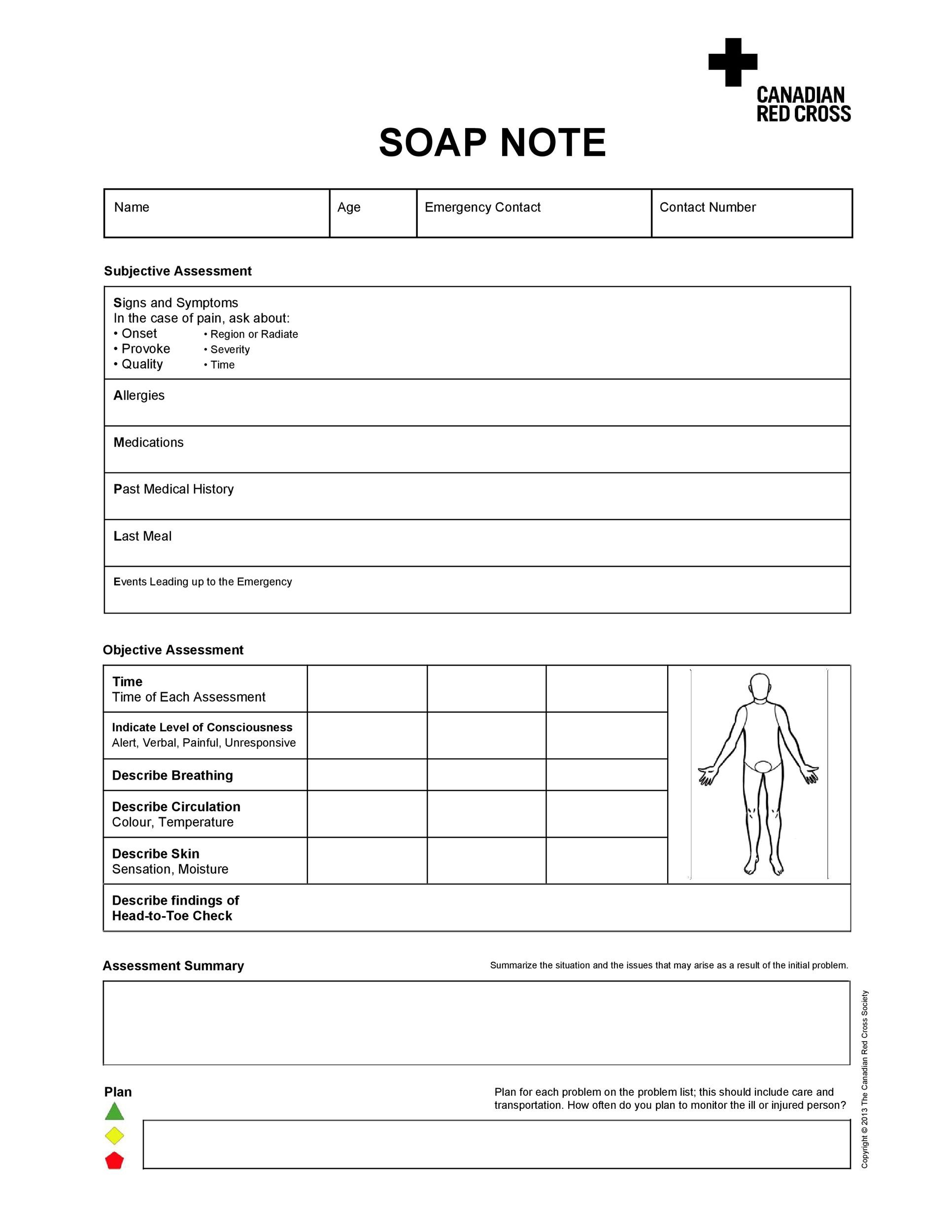
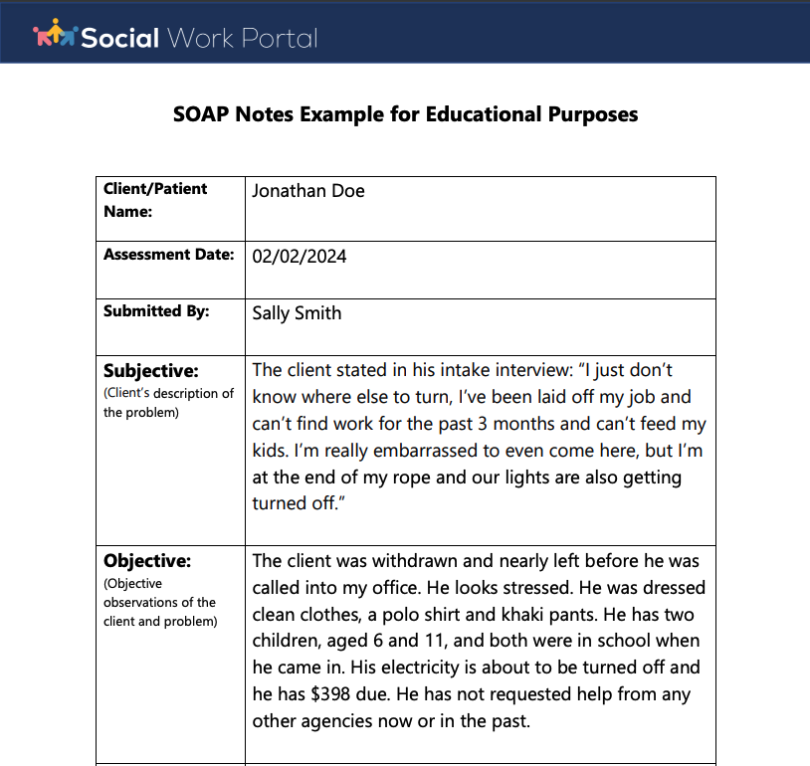
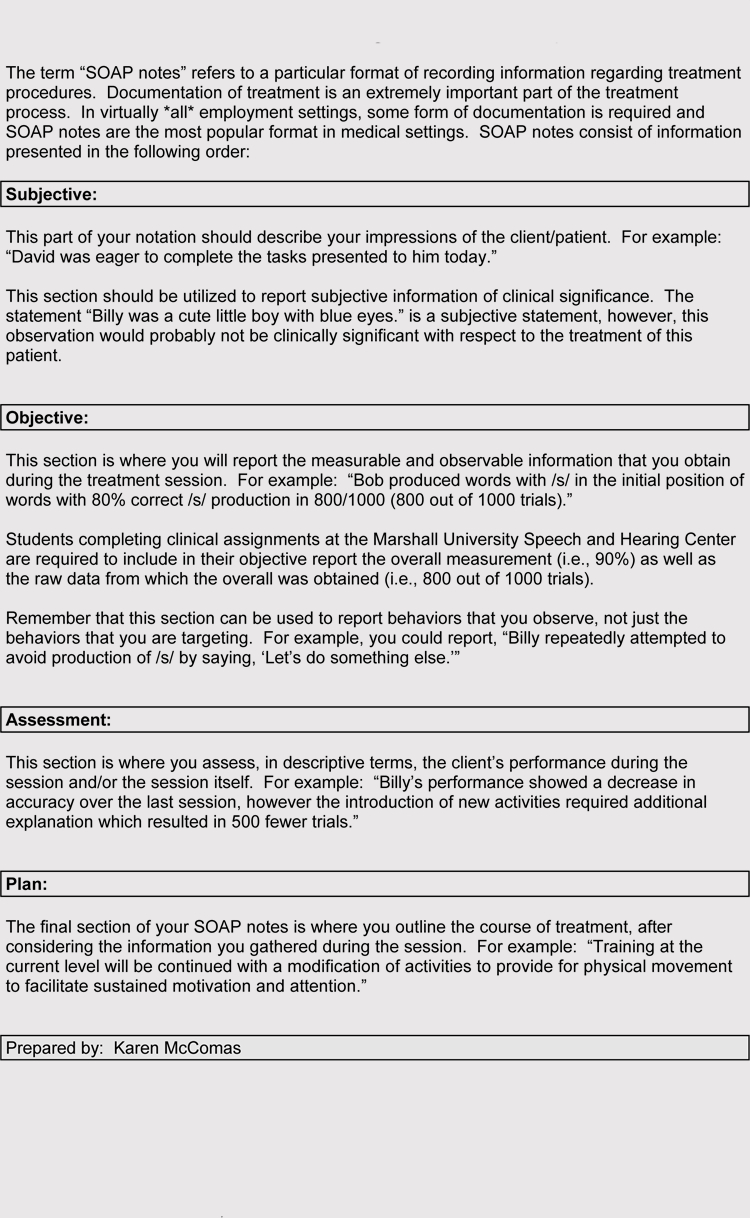
This section captures the patient’s perspective and describes their chief complaint, current symptoms, and relevant medical history. It’s the “story” the patient tells, including their feelings, perceptions, and any information they convey. Examples of what belongs here include the patient’s main reason for the visit (e.g., “sharp pain in lower back for three days”), onset of symptoms, duration, intensity (e.g., “pain is 7/10 on a scale of 0-10”), aggravating or alleviating factors, and relevant social or family history volunteered by the patient. The subjective data is crucial for understanding the patient’s experience and guiding the subsequent objective assessment.

The objective section contains measurable, observable, and verifiable data collected by the healthcare professional. This includes vital signs (blood pressure, heart rate, temperature, respiratory rate), physical examination findings, laboratory results, imaging reports, and observations of the patient’s demeanor or gait. This information should be factual and free of personal bias or interpretation. For instance, instead of “patient looks tired,” an objective observation might be “patient appears fatigued, with dark circles under eyes and slow movements.” Precise and accurate objective data provides the factual basis for the clinical assessment.

In the assessment section, the healthcare professional analyzes and interprets the subjective and objective data to formulate a professional opinion. This typically includes a diagnosis or differential diagnoses, a list of potential problems, and the progress of the patient’s condition. The assessment synthesizes the information from the first two sections, explaining the practitioner’s clinical reasoning. It often includes an explanation of how the patient’s symptoms and objective findings relate to a specific condition or problem, along with a statement about the severity and prognosis. This section demonstrates the clinician’s critical thinking.
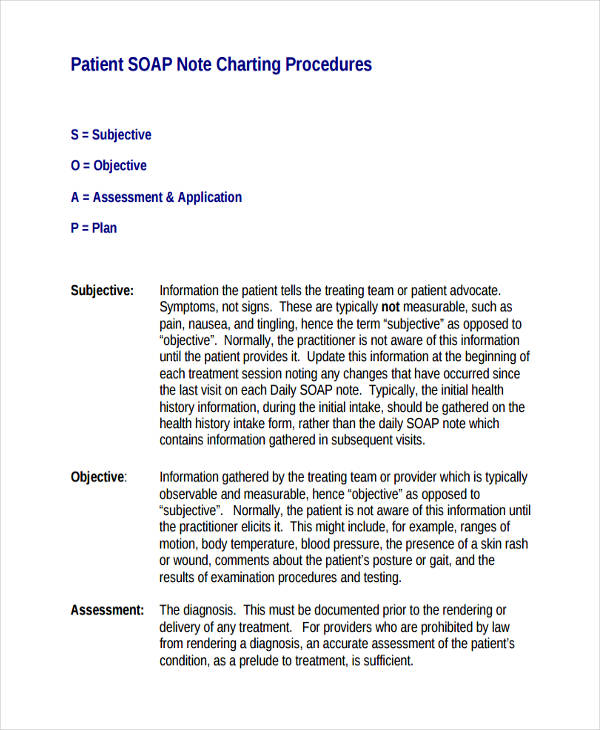
The plan outlines the proposed course of action based on the assessment. This section details what the healthcare professional intends to do to address the patient’s problems. It can include medication prescriptions, referrals to specialists, therapeutic interventions (e.g., physical therapy), diagnostic tests (e.g., blood work, X-rays), patient education, and follow-up instructions. Each element of the plan should be specific, measurable, achievable, relevant, and time-bound (SMART). A well-articulated plan ensures continuity of care and guides subsequent patient encounters, making it clear what steps are being taken and why.

A well-designed Soap Report Template is more than just a blank form; it’s a strategic tool that guides thorough documentation. While the fundamental S.O.A.P. structure remains consistent, the specific fields and prompts within each section can vary based on the discipline and the template’s design. However, certain core components are universally beneficial in creating a robust and functional template.
A comprehensive template for the Subjective section should include dedicated spaces for:
* Chief Complaint (CC): A concise statement in the patient’s own words describing the primary reason for the visit.
* History of Present Illness (HPI): Detailed exploration of the CC using elements like onset, location, duration, characteristics, aggravating/alleviating factors, radiation, temporal patterns, and severity (OLD CARTS).
* Past Medical History (PMH): Relevant past diagnoses, surgeries, hospitalizations, and chronic conditions.
* Medications: Current medications, dosages, and frequency, including over-the-counter drugs and supplements.
* Allergies: Documenting all known allergies and reactions (e.g., drug, food, environmental).
* Social History: Information on lifestyle factors such as smoking, alcohol use, drug use, occupation, living situation, and support system.
* Family History: Relevant familial medical conditions that may impact the patient’s health.
* Review of Systems (ROS): A systematic inquiry about symptoms pertaining to different body systems, often presented as a checklist.
The Objective section of the template should facilitate the recording of empirical data:
* Vital Signs: Structured fields for temperature, pulse, respiratory rate, blood pressure, oxygen saturation, and pain level.
* General Appearance: Observations of the patient’s overall presentation, e.g., “well-nourished, alert, no acute distress.”
* Physical Exam Findings: Organized sub-sections for head, eyes, ears, nose, throat (HEENT), cardiovascular, pulmonary, abdominal, musculoskeletal, neurological, dermatological, and psychiatric exams. These often include checkboxes or brief entry fields for specific findings.
* Lab Results: A section to note relevant lab values or reference to electronic lab records.
* Imaging Reports: Space to summarize findings from X-rays, MRIs, CT scans, etc.
* Other Diagnostic Tests: Any other tests performed and their results.
The Assessment section needs to guide the clinician in interpreting the data. Template prompts might include:
* Diagnosis (Dx): Space for primary diagnosis and any secondary diagnoses, often with ICD-10 codes.
* Problem List: A numbered list of current and active problems the patient is facing.
* Differential Diagnoses: A list of other possible conditions considered.
* Clinical Reasoning/Interpretation: A free-text area or guided prompts for explaining the connection between subjective/objective data and the diagnoses.
* Severity/Prognosis: A brief statement about the current state of the condition and anticipated course.
The Plan section of the Soap Report Template should ensure all aspects of patient management are covered:
* Medications: Prescriptions, including drug name, dosage, route, frequency, and duration.
* Therapeutic Interventions: Referrals to other specialists (e.g., physical therapy, counseling), wound care, diet modifications.
* Diagnostic Orders: Upcoming lab tests, imaging studies, or other diagnostic procedures.
* Patient Education: Information provided to the patient about their condition, medications, lifestyle changes, or self-care.
* Follow-up: Specific instructions for the next appointment, including timing and purpose.
* Referrals: Details of any referrals made.
* Consults: Any consultations requested with other providers.
By including these core components, a template can ensure comprehensive, consistent, and high-quality documentation across various healthcare settings.
The implementation of a standardized Soap Report Template offers a multitude of advantages that extend beyond mere record-keeping, impacting patient care, operational efficiency, and legal protection within healthcare settings. The structured nature of these templates transforms what could be a fragmented process into a cohesive and reliable system.
One of the primary benefits is improved clarity and readability. When all practitioners use the same format, notes become predictable and easier to navigate. This consistency significantly reduces the time required for clinicians to locate specific information, allowing them to quickly grasp the patient’s current status, history, and treatment plan. This clarity is vital in fast-paced environments where quick decisions are often necessary.
Furthermore, a standardized template fosters enhanced communication among healthcare professionals. In multi-disciplinary teams, where various specialists contribute to a patient’s care, a uniform documentation style ensures that every team member can understand the notes from others. This seamless exchange of information minimizes misinterpretations and prevents crucial details from being overlooked, thereby promoting truly collaborative care.
From a legal standpoint, using a template provides stronger legal protection and compliance. Comprehensive and consistently formatted notes serve as a robust legal record, demonstrating that appropriate care was rendered and that all necessary steps were taken. In the event of a medical malpractice claim or audit, well-structured SOAP notes can provide undeniable evidence of due diligence and adherence to professional standards, making it harder for gaps or inconsistencies to be exploited.
The template also contributes significantly to a streamlined workflow and increased efficiency. By guiding the practitioner through each required section, it reduces the cognitive load associated with remembering what information to include. This often leads to faster, more complete documentation at the point of care, freeing up valuable time that can be redirected toward direct patient interaction or other clinical tasks. Over time, this efficiency can translate into significant operational savings and improved clinic throughput.
Ultimately, the most profound benefit lies in its direct impact on better patient care and outcomes. By ensuring that all critical information is consistently captured and easily accessible, the template supports more informed decision-making. Clinicians can track progress more effectively, identify trends, and adjust treatment plans based on a complete and accurate picture of the patient’s health. This systematic approach reduces the likelihood of errors, improves continuity of care, and ultimately leads to safer and more effective treatment experiences for patients.
While the core Subjective, Objective, Assessment, and Plan components of a SOAP note remain universal, the specific details and emphasis within each section must be tailored to the unique requirements of different healthcare disciplines. A generic Soap Report Template is a good starting point, but customization is key to maximizing its utility for specialists.
For instance, in physical therapy, the Objective section would place a heavy emphasis on measurable functional assessments. This might include specific fields for range of motion (ROM) measurements, muscle strength grading (e.g., using a 0-5 scale), gait analysis, balance tests (e.g., Berg Balance Scale), and posture observations. The Plan section would detail specific exercises, manual therapy techniques, modalities used, and home exercise program instructions, along with clear functional goals.
In mental health, the Subjective section would be significantly expanded to capture detailed psychological symptoms, social stressors, emotional state, coping mechanisms, and risk assessments (e.g., suicidal or homicidal ideation). The Objective section might include observations of affect, thought process, speech patterns, and mental status exam findings. The Assessment would focus on specific psychiatric diagnoses (e.g., Major Depressive Disorder, Generalized Anxiety Disorder) and a formulation of the case. The Plan would outline therapeutic interventions, medication management, crisis planning, and referrals to social services or other specialists.
Nursing documentation often requires a broader scope, encompassing vital signs, pain assessment, wound care details, medication administration, patient education provided, and observations related to activities of daily living (ADLs). A nursing-specific template might integrate flow sheets for repeated observations, medication reconciliation checklists, and dedicated sections for patient education topics. Their plan often revolves around continuous monitoring, administering treatments, and ensuring patient comfort and safety.
For chiropractic care, the Objective section would focus on spinal alignment, palpation findings, muscle spasm, neurological screen results, and orthopedic tests. The Assessment would articulate chiropractic diagnoses (e.g., subluxation complexes) and their relationship to the patient’s symptoms. The Plan would detail specific adjustments performed, adjunctive therapies (e.g., heat, ice, electrical stimulation), and ergonomic advice.
Even within primary care, customization is vital. A template for a routine check-up might include preventative screening checklists and vaccine administration records. For chronic disease management, it would emphasize adherence to specific guidelines, monitoring parameters, and patient self-management goals. The importance of tailoring the template lies in its ability to prompt the clinician for the most relevant information for their specific practice, ensuring comprehensive yet concise documentation that reflects the nuances of their specialty. This customization enhances relevance, efficiency, and the overall quality of care.
Implementing and optimizing a Soap Report Template requires more than just distributing a new form; it involves strategic planning, training, and ongoing evaluation. A thoughtful approach ensures smooth adoption and maximal benefit from this crucial documentation tool.
The first step is choosing the right format. For many practices, a digital template integrated within an Electronic Health Record (EHR) or Electronic Medical Record (EMR) system is ideal. Digital templates offer advantages like auto-population of patient data, standardized drop-down menus, easy searchability, and seamless integration with billing and scheduling systems. However, for smaller practices or specific scenarios, a well-designed printable PDF template or even a structured notebook might suffice. The choice should align with the practice’s technological capabilities, budget, and workflow.
Once the format is selected, training staff is paramount. All healthcare professionals who will be using the template must receive thorough instruction on how to complete each section accurately and consistently. This training should cover the rationale behind SOAP notes, the specific expectations for each field in the template, and practical examples. Role-playing or mock documentation sessions can be highly effective. Emphasize the importance of clear, concise, and objective language, and educate them on common pitfalls to avoid.
Regular review and updates are essential for optimization. The healthcare landscape is dynamic, with evolving best practices, new regulations, and changes in patient demographics. Periodically, gather feedback from users on the template’s usability, completeness, and efficiency. Are there sections that are rarely used or consistently missed? Are there new types of information that need to be captured? Use this feedback to refine the template, adding or modifying fields as needed to ensure it remains relevant and effective.
Finally, integration with existing EHR/EMR systems is crucial for digital templates. Ensure that the template is correctly mapped to the system’s data fields to prevent redundant data entry and improve data flow. This integration can automate tasks like populating patient demographics, ordering labs, and generating prescriptions directly from the SOAP note, further enhancing efficiency and accuracy. When implemented thoughtfully and optimized continuously, a Soap Report Template becomes an indispensable asset, supporting high-quality care and efficient operations.
While a Soap Report Template is designed to simplify and standardize documentation, certain common mistakes can undermine its effectiveness and potentially compromise patient care or legal standing. Being aware of these pitfalls is the first step toward avoiding them and maximizing the template’s benefits.
One frequent error is lack of detail in subjective complaints. Simply writing “patient has pain” is insufficient. The template prompts should encourage capturing the full story, including the pain’s onset, location, duration, character, aggravating/alleviating factors, radiation, temporal patterns, and severity (OLD CARTS). Skipping these details can lead to an incomplete understanding of the patient’s condition.
Another common mistake is subjectivity creeping into the objective section. The objective section must contain only measurable and observable facts. Phrases like “patient seems anxious” or “looks like they are in pain” are interpretations, not objective findings. Instead, document observable signs such as “patient restless, wringing hands, states heart palpitations” or “grimacing with movement, guarding affected limb.” Maintaining strict objectivity ensures the factual integrity of the notes.
Vague assessments are also problematic. An assessment should clearly articulate the diagnosis or differential diagnoses and provide a concise interpretation of how the subjective and objective data support this conclusion. Avoiding definitive statements or providing a weak rationale for the diagnosis reduces the clarity and usefulness of the note. The assessment should demonstrate clear clinical reasoning.
Similarly, unclear or incomplete plans can lead to fragmented care. A plan must be specific, measurable, achievable, relevant, and time-bound (SMART). Vague instructions like “continue meds” or “follow up as needed” are insufficient. Instead, specify “continue gabapentin 300mg TID, follow up in 2 weeks for reassessment of neuropathic pain.” Every element of the plan—medications, diagnostics, referrals, patient education, and follow-up—should be explicitly detailed.
Finally, a critical but often overlooked error is failing to sign and date entries promptly. All documentation, especially in a legal record like a patient chart, must be authenticated and dated by the person making the entry. Late entries should be clearly marked as such. This ensures accountability and maintains the integrity of the medical record. Adhering to these best practices will ensure that the Soap Report Template serves its intended purpose effectively and reliably.
The Soap Report Template stands as an indispensable tool in modern healthcare, fundamentally transforming the way patient information is documented and utilized. Its structured framework, encompassing Subjective, Objective, Assessment, and Plan, provides a standardized and comprehensive method for capturing critical clinical data, ensuring consistency and clarity across diverse medical disciplines. From enhancing communication among healthcare professionals to providing robust legal protection and streamlining workflow, the benefits of adopting a well-implemented template are profound and far-reaching.
By promoting meticulous detail in patient narratives, objective observations, precise diagnostic assessments, and actionable treatment plans, the template significantly contributes to improved patient safety and elevated standards of care. Customization allows it to serve the unique needs of various specialties, from mental health to physical therapy, ensuring its relevance and effectiveness across the entire healthcare spectrum. Through diligent implementation, continuous optimization, and conscious avoidance of common documentation pitfalls, healthcare providers can leverage the full potential of this powerful tool. The Soap Report Template is not merely a form; it is a cornerstone of efficient, ethical, and high-quality patient care, supporting informed decision-making and fostering a culture of excellence in medical documentation.