This document outlines the essential components of effective record-keeping in psychotherapy. Accurate and thorough documentation is not just a regulatory requirement; it’s a cornerstone of quality patient care, facilitating continuity of treatment, legal protection, and ongoing clinical improvement. A vital tool in this process is a well-structured psychotherapy progress note template. This article will explore what constitutes a comprehensive progress note, different template options, best practices for writing them, and the importance of adapting these notes to individual client needs. We’ll delve into the various sections that should be included, offer examples, and address common challenges therapists face when documenting sessions. Understanding and utilizing a robust progress note system can significantly enhance the therapeutic process and contribute to a more professional and ethically sound practice.
A psychotherapy progress note is a written record of a therapy session, documenting the client’s progress, concerns, interventions used, and any relevant observations. It serves as a crucial communication tool among members of the treatment team, whether that’s a therapist, psychiatrist, or other healthcare providers. Progress notes are not simply summaries of what happened in a session; they are active documents that reflect the therapist’s clinical judgment and ongoing assessment of the client’s well-being. They provide a historical context for treatment, allowing therapists to track changes over time and adjust their approach as needed. Furthermore, these notes are essential for legal and ethical reasons, protecting both the therapist and the client by maintaining a clear record of services provided and the rationale behind treatment decisions. Failing to maintain accurate and detailed progress notes can lead to serious consequences, including legal liability and compromised client care.
The importance of progress notes extends far beyond simple record-keeping. Several key factors underscore their significance:
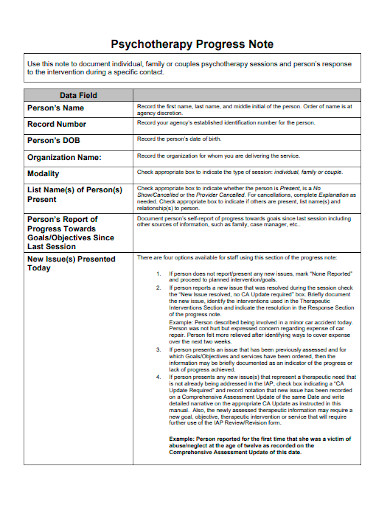
A comprehensive progress note typically includes the following key components. While the specific format may vary depending on the therapist’s preferences and the requirements of their practice or insurance provider, these elements are generally considered essential.
The date and time of the session are foundational elements. This information ensures accurate chronological tracking of the client’s treatment history.
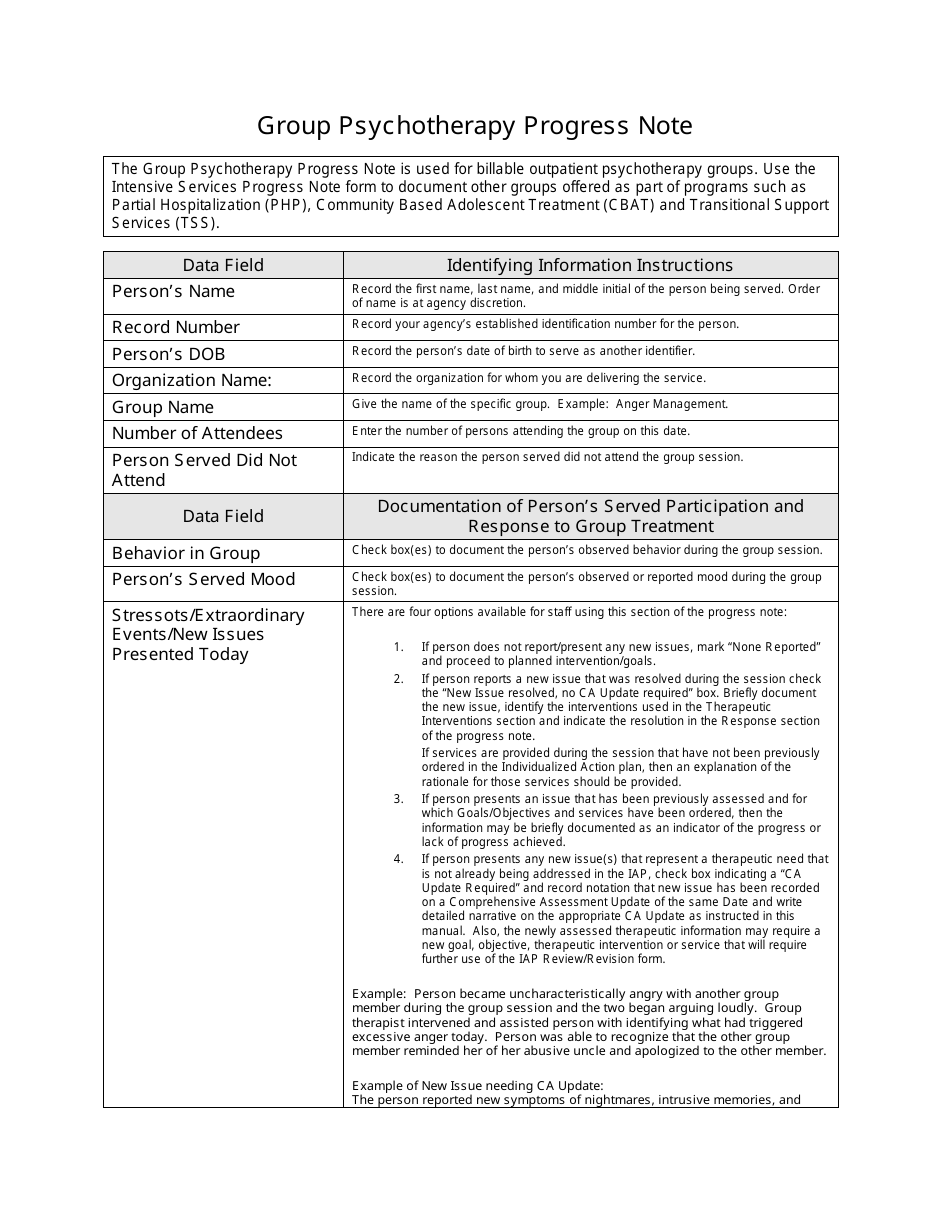
This section includes the client’s full name, date of birth, and any relevant identifying information, such as their client ID. This information should be consistent with the client’s intake paperwork and updated as needed.
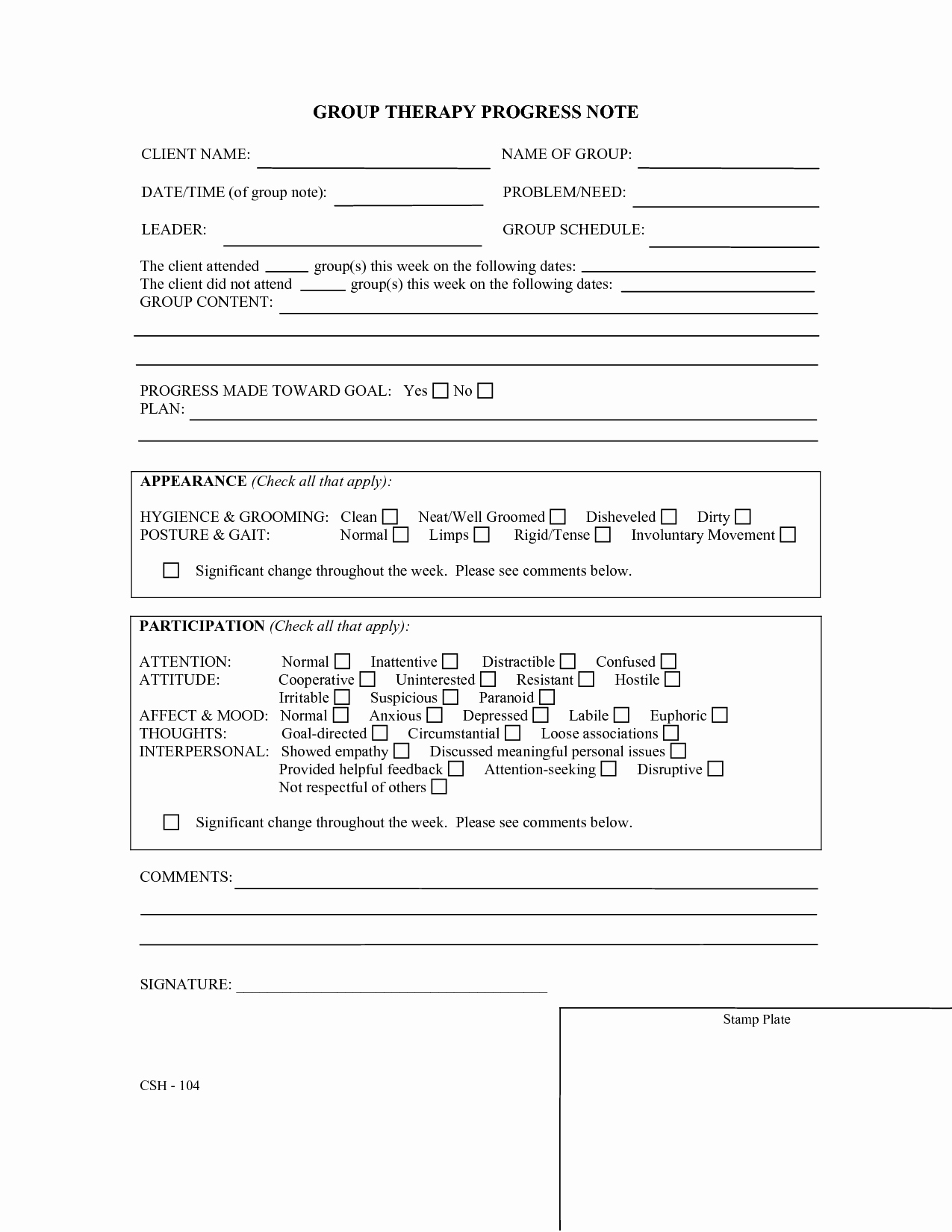
Specify the type of session conducted (e.g., individual therapy, couples therapy, family therapy).

Record the duration of the session.
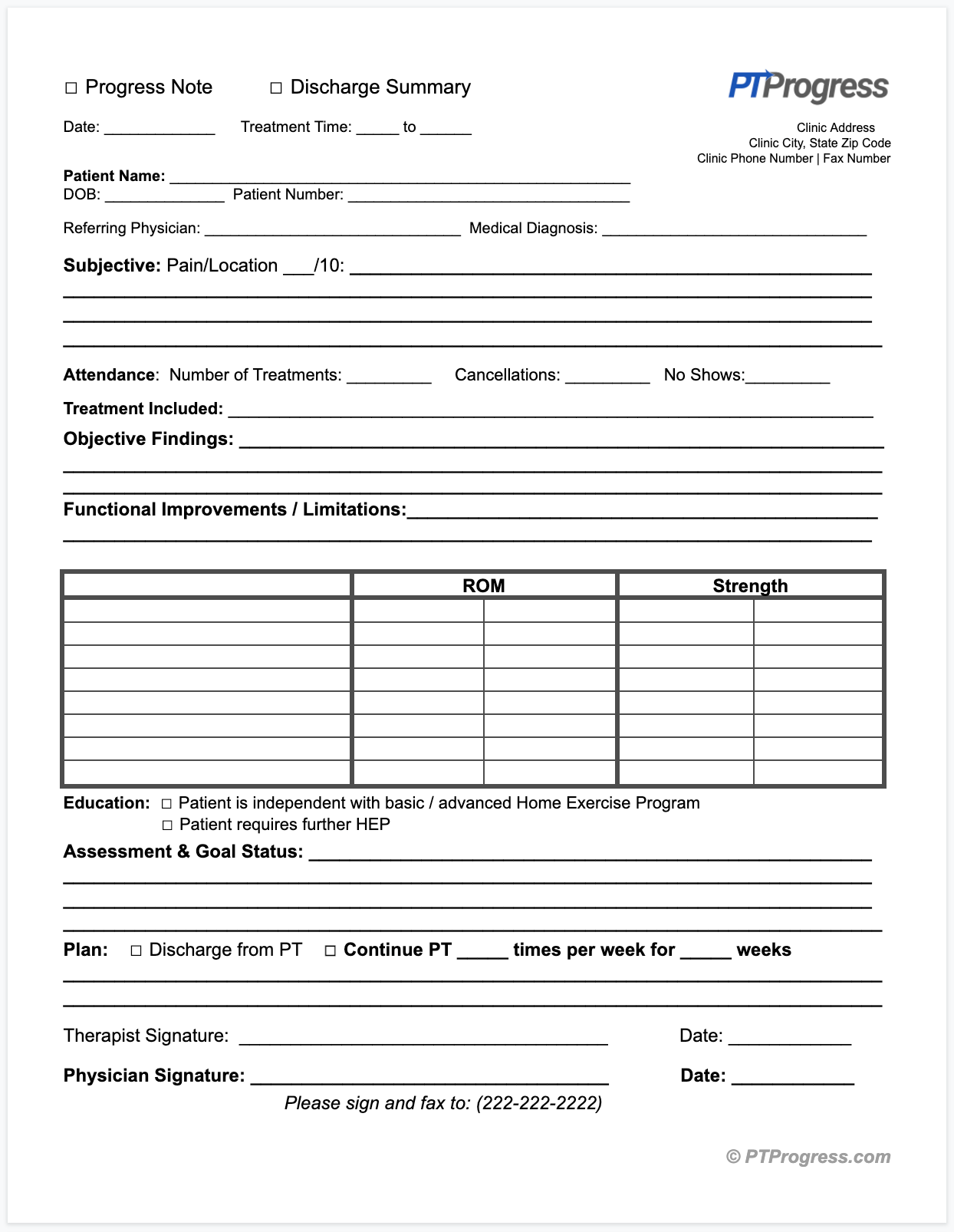
This is a crucial section that outlines the client’s primary concerns and the issues discussed during the session. Use the client’s own words whenever possible to capture their perspective. Summarize the key issues they brought up and any changes in their presentation since the last session.
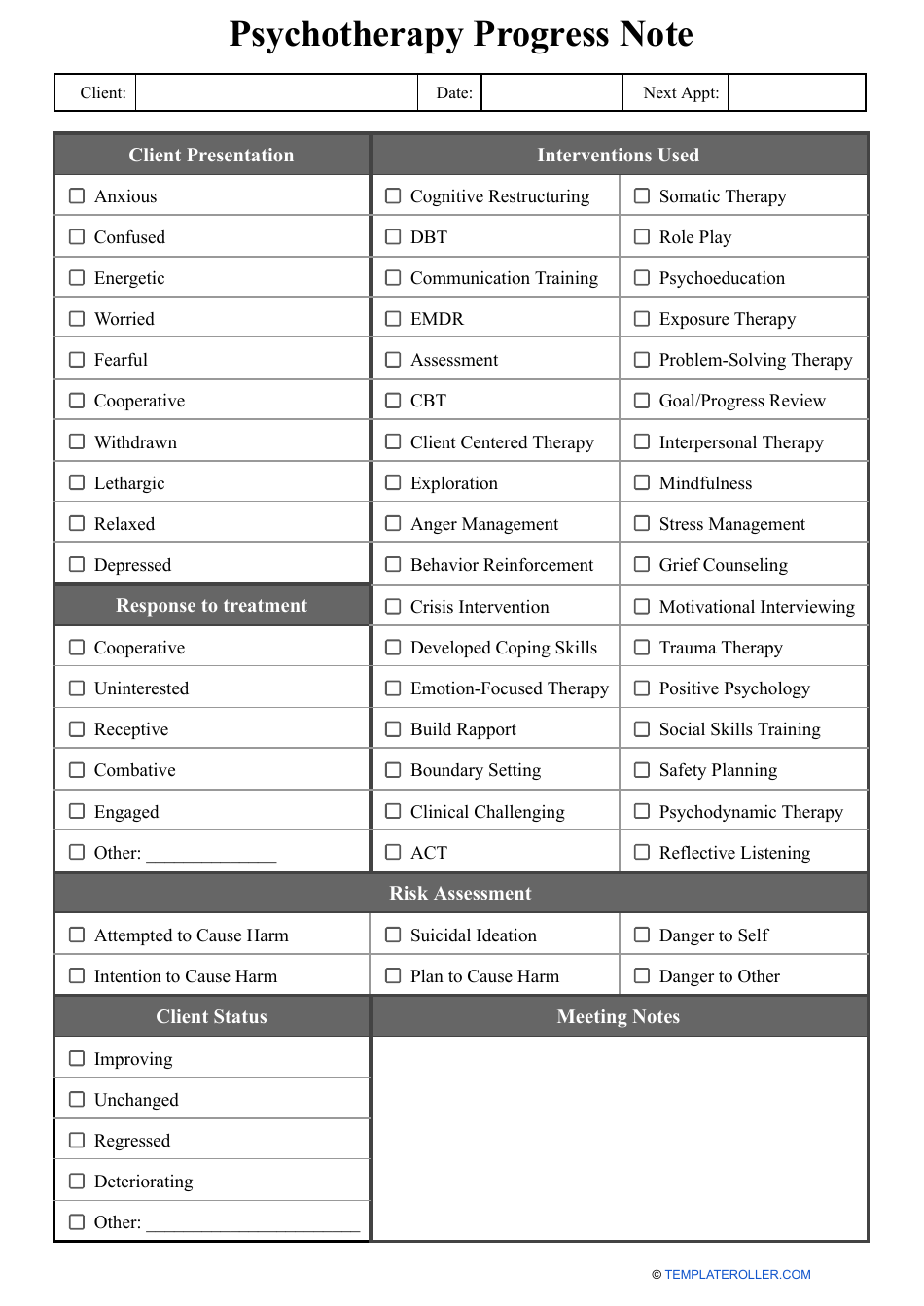
Detail the specific therapeutic techniques or interventions used during the session. This might include cognitive behavioral techniques, mindfulness exercises, motivational interviewing, or other approaches. Explain why you chose to use those specific interventions.
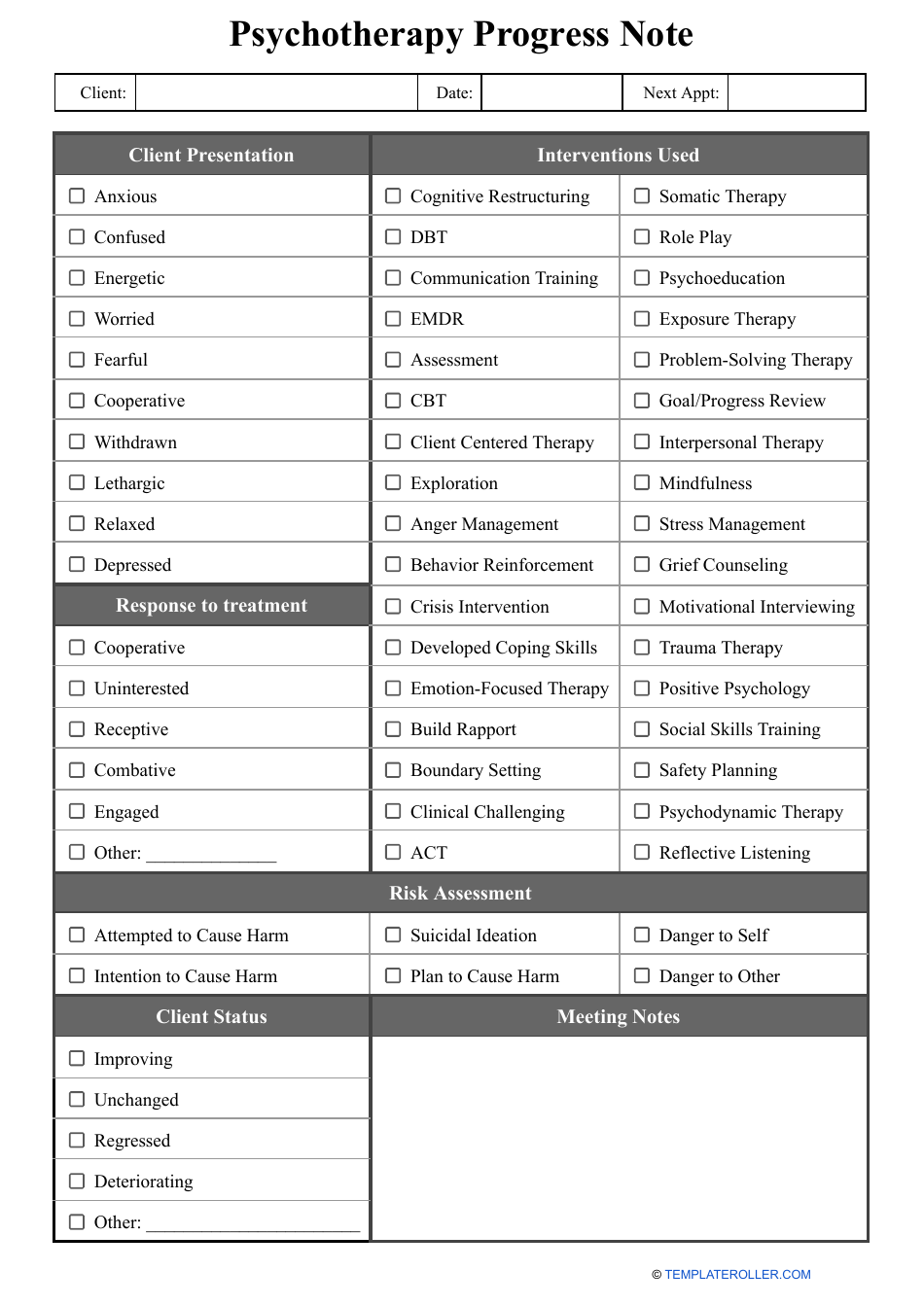
Describe the client’s response to the interventions used. Did they engage positively? Were they resistant? How did they react emotionally? Document any observed changes in their behavior, mood, or thought patterns.

Assess the client’s progress towards their treatment goals. Are they making progress? Are there any obstacles hindering their advancement? This section is crucial for tracking effectiveness and adjusting the treatment plan.
Outline the plan for the next session, including any specific tasks or assignments for the client, any changes to the treatment plan, and the proposed focus of the next session.
Include your professional impressions of the client’s current state. This may involve summarizing your clinical assessment of their emotional state, cognitive functioning, and overall well-being.
Numerous psychotherapy progress note template options are available, each catering to different therapeutic modalities and practice preferences. The choice of template should align with the therapist’s individual style and the specific needs of their clients.
This is the most common type of progress note template, presenting information in a chronological order, typically starting with the most recent session. It’s easy to use and provides a clear timeline of the client’s treatment.
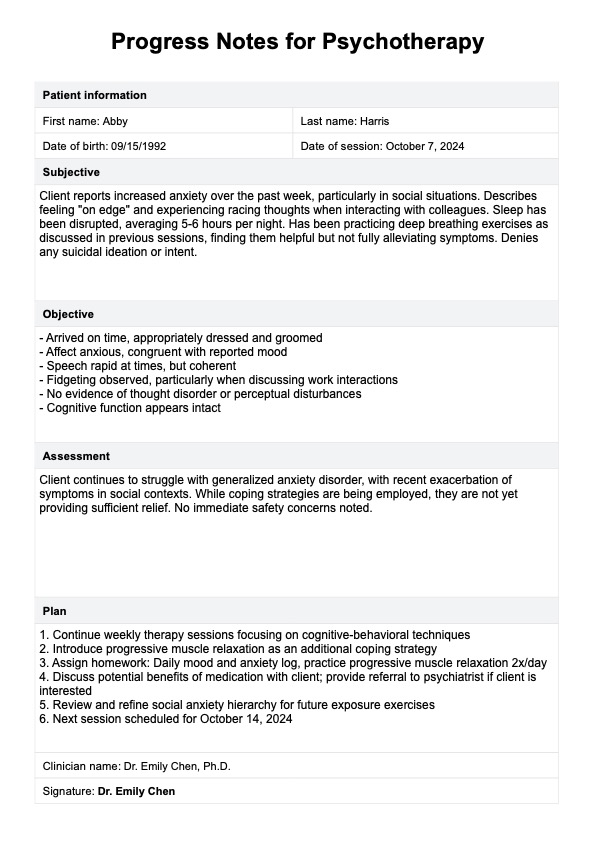
The SOAP template is a widely used format that stands for Subjective, Objective, Assessment, and Plan. This template provides a structured approach to note-taking, ensuring that all relevant information is captured.
* Subjective: Client’s reported experiences, feelings, and concerns.
* Objective: Observable behaviors and data gathered during the session.
* Assessment: Therapist’s clinical interpretation of the information.
* Plan: The next steps in treatment.
The BIRP template stands for Behavior, Intervention, Response, and Plan. This template focuses on the specific actions and outcomes of the session.
A condensed version of the SOAP template, ideal for therapists who need to document quickly and efficiently.
Following best practices can ensure that your progress notes are accurate, comprehensive, and effective.
Focus on documenting observable behaviors and client statements rather than subjective opinions or interpretations. Use the client’s own words whenever possible.
Avoid vague or general statements. Provide specific details about the client’s concerns, the interventions used, and their response.
Write progress notes as soon as possible after the session, while the details are still fresh in your mind. This will improve the accuracy and completeness of your documentation.
Maintain a professional and objective tone. Avoid using judgmental or biased language.
Avoid jargon or technical terms that may not be easily understood by others. Use clear and concise language to communicate effectively.
Be aware of the legal and ethical requirements for documentation in your jurisdiction and adhere to them strictly. This includes protecting client confidentiality and avoiding the inclusion of irrelevant or inappropriate information.
While templates provide a useful framework, it’s important to adapt them to meet the specific needs of each client. Some clients may require more detailed documentation than others. Consider the following factors when adapting your psychotherapy progress note template:
Therapists often face challenges when writing progress notes. Some common challenges include:
Effective documentation is an integral part of providing quality psychotherapy. A well-utilized psychotherapy progress note template promotes continuity of care, provides legal protection, facilitates clinical improvement, and upholds ethical obligations. By understanding the essential components of a progress note, choosing the right template, and adhering to best practices, therapists can ensure that their documentation is accurate, comprehensive, and beneficial for both themselves and their clients. Remember to adapt your notes to meet the unique needs of each client and to regularly review and refine your documentation system. Investing time and effort in creating a robust progress note system ultimately enhances the therapeutic process and contributes to better outcomes for clients.